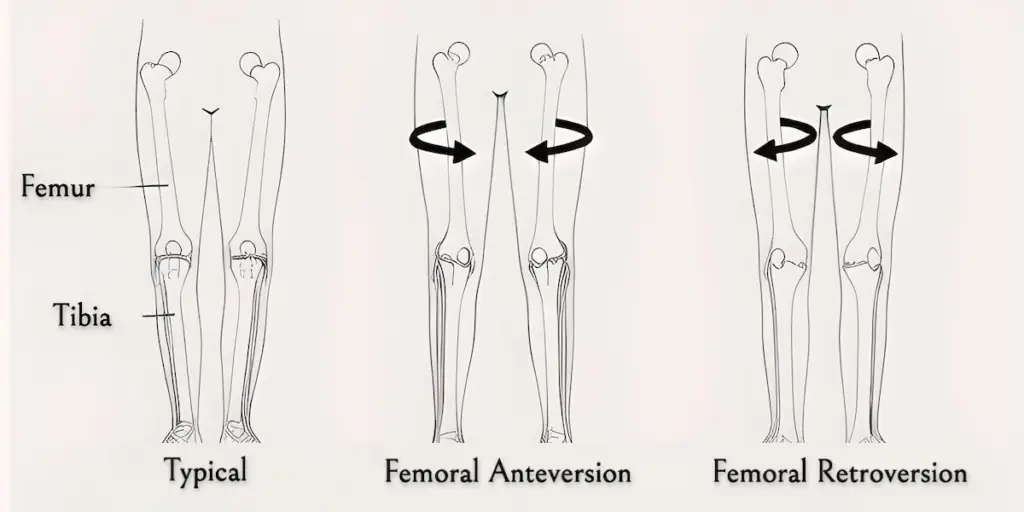
In this study in the journal Knee Surg Sports Traumatol Arthrosc. (KSSTA), Chen, et al. evaluated CT scans of patients with and without patellar instability. Not surprisingly, the patients with unstable knee caps had worse alignment as measured by tibial tubercle-trochlear groove (TT-TG), (20.1 versus 15.6). Perhaps more interesting, they found that patients with patellar instability had significantly more femoral anteversion angle (FAA) (21.6 versus 10.6).
Studies like this may ultimately help us determine which patients need surgery and which patients can get away with physical therapy after a patellar dislocation. Evaluation of the hip is very important in assessing a patient with patellar instability and can easily be overlooked.
Read more in this KSSTA journal study.