Quick Summary
A distalizing tibial tubercle osteotomy (TTO) lowers a high-riding kneecap (patella alta) by detaching a small block of bone from the front of the tibia and reattaching it in a more anatomically correct position. The procedure relieves chronic anterior knee pain, fat pad impingement, patellar tendinitis, and inferior patellar cartilage wear, and can also stabilize a kneecap that dislocates. Modern fixation techniques have substantially reduced the historical risks of fracture and non-union when performed by an experienced patellofemoral surgeon.
A relatively rare operation as far as knee surgery goes is a distalizing tibial tubercle osteotomy. I do this surgery for patients who have patella alta or high knee caps. This can result in chronic anterior knee pain, fat pad impingement, patellar tendinitis and inferior patellar cartilage wear. It can also contribute to patellar instability in some patients.
The surgical treatment has historically been associated with significant complications such as fracture, delayed union or non-union or failure to unite. This modification of the technique is how I have been doing this surgery for the past 6-7 years and has resulted in a lot of satisfied patients.
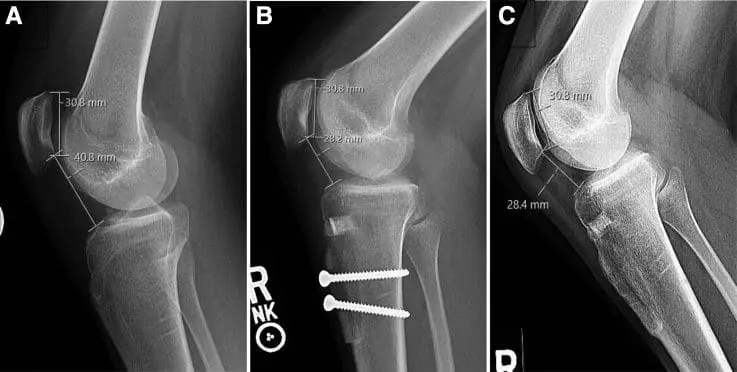
The image shows lateral radiographs of the right knee from a 19-year-old female patient with patella alta and patellar instability who was indicated for tibial tubercle osteotomy with distalization.
Read more in Arthroscopy Techniques.
What Is Patella Alta and Why Does It Need Surgical Correction?
Patella alta — or a high-riding kneecap — is an anatomical variation in which the patella sits abnormally high relative to the trochlear groove of the femur, reducing bony engagement and predisposing the joint to instability and pain. Because the kneecap is "perched" above the groove during early flexion, the soft tissues take on a disproportionate share of the load, leading to chronic anterior knee pain, fat pad impingement, patellar tendinitis, inferior patellar cartilage wear, and recurrent patellar instability in some patients.
When non-operative care — activity modification, focused physical therapy, bracing, and addressing soft-tissue imbalance — fails to restore stability or relieve pain, surgical correction of the bony anatomy may be indicated. A distalization tibial tubercle osteotomy directly addresses the height of the patella by moving the tubercle (and therefore the patellar tendon attachment) further down the tibia, restoring more normal patellofemoral mechanics.
How the Distalization TTO Procedure Works
During a distalizing TTO, a precise block of bone containing the tibial tubercle is detached from the front of the tibia, repositioned distally (and sometimes medialized), and rigidly fixed with screws so the patella now tracks correctly through the trochlear groove. The modification of the technique used at HSS prioritizes a long bone block, controlled cuts, and rigid fixation, which together support reliable bone-to-bone healing.
The osteotomy is often combined with other patellofemoral procedures — such as MPFL reconstruction for ligament instability or cartilage restoration when an inferior pole lesion is present — based on the patient's underlying anatomy. Surgical planning relies on weight-bearing X-rays for patellar height, MRI for cartilage and ligament status, and CT in selected cases to measure tibial tubercle–trochlear groove (TT–TG) distance.
Risks and Complications
Like any orthopedic procedure, a distalizing TTO carries real risks — historically including tibial fracture, delayed union or non-union of the bone block, infection, hardware irritation, blood clots, stiffness, and recurrent instability when underlying anatomic factors are not fully addressed. Modern fixation strategies and careful patient selection have substantially reduced complication rates compared with earlier techniques, but no procedure is risk-free, and outcomes depend on diagnosis, anatomy, and adherence to the post-op rehabilitation plan.
This is one of the reasons distalization is reserved for patients in whom patella alta is clearly contributing to symptoms and where conservative care has been exhausted — not as a first-line treatment.
Recovery and Rehabilitation
Recovery after a distalizing TTO typically involves a period of protected weight bearing, knee bracing, and structured physical therapy, with most patients walking unassisted by 6–8 weeks and returning to higher-impact activities by 4–6 months as the bone block fully heals. Timelines are individualized based on bone healing, concurrent procedures, and the patient's pre-operative function.
Adherence to the rehab program is one of the strongest predictors of a successful outcome — underloading the bone block too early risks loss of fixation, while pushing too aggressively can aggravate anterior knee pain.
Key Takeaways
- Distalization TTO addresses the bony cause of patella alta — not just the symptoms.
- Modern fixation techniques have substantially reduced the historical risks of fracture and non-union.
- The procedure is often combined with MPFL reconstruction or cartilage restoration based on the patient's specific anatomy.
- Outcomes are best when the operation is performed by a fellowship-trained patellofemoral specialist.
If you have been diagnosed with patella alta or recurrent patellar instability and would like a personalized evaluation, learn more about joint preservation osteotomy or contact the office to schedule a consultation with Dr. Strickland.
Frequently Asked Questions
Who is a candidate for a distalizing TTO?
A distalizing TTO is generally indicated for patients with symptomatic patella alta — confirmed on imaging — who have failed structured non-operative treatment and who continue to experience anterior knee pain, fat pad impingement, patellar tendinitis, inferior patellar cartilage wear, or recurrent kneecap instability. The decision is individualized based on patellar height (Caton-Deschamps Index, Insall-Salvati ratio), trochlear morphology, alignment, and overall function.
How long does the surgery take and what is the hospital stay?
A distalizing TTO is typically performed as a same-day or short-stay procedure, often taking 1.5–3 hours depending on whether additional procedures — such as MPFL reconstruction or cartilage restoration — are performed at the same time. Most patients go home the day of surgery in a knee brace with crutches.
When can I return to sports after a distalization TTO?
Return to higher-impact activities and sports is typically targeted at 4–6 months postoperatively, once the bone block has fully healed and quadriceps strength, range of motion, and patellar tracking have been restored. The exact timing depends on bone healing on imaging, completion of structured rehabilitation, and any concurrent procedures.
Will the screws need to be removed later?
Hardware removal is not routine, but the screws used to fix the bone block can become symptomatic in a subset of patients — particularly thin individuals where the screw heads can be palpable or irritate when kneeling. If hardware is symptomatic after the bone has fully healed, removal can be discussed as a separate, smaller outpatient procedure.
Is a distalization TTO the same as an anteromedialization (AMZ) TTO?
No — both are tibial tubercle osteotomies, but they correct different problems. A distalization moves the tubercle "down" the tibia to address patella alta, while an anteromedialization (Fulkerson) shifts the tubercle medially and forward to offload an isolated lateral or distal patellar cartilage lesion. The two can also be combined when patients have both excessive patellar height and a maltracking pattern that needs to be unloaded.